It’s the challenge facing every business in the current financial climate – how to maintain levels of quality, even improve them, while keeping down costs? In this article, improvement specialist and head of services practice at Newton Europe, CHRISTIAN HANSEN, discusses this dilemma
For those in local government, the NHS, and other service providers, this often fraught balancing act between improving services and controlling spend becomes particularly challenging. Yet, they can be balanced.
In most businesses all things being equal, service level is influenced directly by resources employed or cost – in other words, the quality of the service is contingent on how much funding it has received. For the likes of a council service helpline, this may mean that increasing the number of call handlers will reduce call waiting times. But, in frontline health services, a more apposite example may be that increasing the number of clinicians helps to reduce accident and emergency waiting times. It could mean the difference between seeing a clinician immediately, or having to wait, and patients getting the treatment they need when they need it.
There is a common misconception that cost-cutting is by definition a retrograde step and will lead inevitably to a reduction in service levels
In difficult economic times, reducing costs and driving efficiencies is a real necessity. There is a common misconception that cost-cutting is by definition a retrograde step and will lead inevitably to a reduction in service levels.
However, low costs and high quality do not have to be strangers passing each other in the night. Indeed, given the right circumstances, they can be happy bedfellows.
Improvement in efficiency is the only way to break this link. If the processes and systems through which they operate are robust, and if staff are fully aware of what is required of them and are able to follow procedures, then quality and quantity will be achieved and the two should not be separated.
Nevertheless, in this situation, there must of course also be a trade-off between monetising the efficiency gain and using it to increase service levels.
Taking a whole systems or total cost of ownership view where all the costs of failure or poor quality are considered, and using a standard cost versus quality model, a new optimum can be delivered, marrying both a reduction in cost and an improvement in quality.
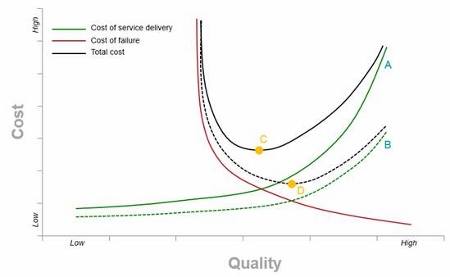
If we consult the chart below, where the cost of service delivery is the solid green line, then the cost grows exponentially as you try and reach perfect quality or service level. For the NHS, this might be seeing every patient as they come through the door, as stated earlier.
Low costs and high quality do not have to be strangers passing each other in the night. Indeed, given the right circumstances, they can be happy bedfellows
The cost of failure is represented by the solid red line. This can include such things as lost sales due to customers going elsewhere after receiving a poor-quality service; further demand being placed on the service as a result of not fully satisfying the client need first time around; service fines and penalties; warranty claims; or compensation and lawsuits.
At some point, quality might be so poor that the service is no longer fit for purpose.
For the likes of the NHS, the true cost of quality is often difficult to quantify because the effects can have a time delay – such as a hip replacement being required in five years rather than 10 due to poor implants. In addition, measures of lost sales are often inaccurate and it is very difficult to correlate them directly to quality. For instance, customers may say they sought out a better quality service when they were actually swayed by the brand or its marketing.
When you aggregate the two, there is an optimal trade-off point between cost of quality and failure that the business should be aiming to operate at – point C on our chart below. In practice, many businesses don’t operate at this point because, while the cost of service delivery is easy to measure, the full cost of failure is often not. It is also usually underestimated.
A successful solution will balance the requirement to reduce costs and improve profitability with the need to deliver superior service with less. The challenge is taking the leap and choosing which solution is best for you
However, by looking at, and improving, operational efficiency, the cost of service delivery can be shifted down and to the right – represented by a shift from point A to point B on the chart. Thus, with the same resources, a higher service level can be delivered, or if the service level is maintained, the cost of delivery can be reduced in a situation where each call handler can now answer more calls per hour. It is often a good idea to approach cost reduction from the perspective of the service user.
When you also factor in the cost of failure - represented by the red line - and assume that this is unchanged, there is a new optimal operating level for the business, found at point D, which is lower in cost and higher in quality.
In the private sector this would give the business a significant advantage over competitors, but has huge potential applications across a much wider platform. As we can see then, attempting to lower costs while maintaining quality levels doesn’t have to be mutually exclusive. A successful solution will balance the requirement to reduce costs and improve profitability with the need to deliver superior service with less. The challenge is taking the leap and choosing which solution is best for you.






